
{kind=link}
Population in Ethiopia:
Based on population projections of the Ethiopia Central Statistical Agency (CSA) for 2016, adolescents and youth in the age range 10 to 29 numbered 38,545,711 (19,466,543 males and 19,079,177 females). This age group accounted for an estimated 42 percent of the total population of Ethiopia, while those aged 10 to 24 are 33 percent of the population. The majority of Ethiopian adolescents and youth reside in rural areas (79 percent of males and 78 percent of females). The percent of adolescents in rural areas increases among those in younger age groups. Among those aged 10 to 14, 81-82 percent are resident in rural areas. Among young people aged 25 to 29, 74-75 percent are resident in rural areas. The trend of increasing urban residence at later ages could be a reflection of rural urban migration during adolescence and youth.
Policy Responses
In order to improve the health and wellbeing of these group of the population, the government of Ethiopia has made a bold commitment to respond to the health needs of the young people. The ministry of health developed and implemented the first national Adolescent and Youth Reproductive health strategy (2006-2015) for almost a decade and a significant improvement on the reproductive health of adolescents and youth particularly among women and girls is recorded. The Health Sector Transformation Plan (HSTP I) recognized the vulnerability and risk of sexual and reproductive health of adolescent and youth in Ethiopia and notify that the lack of access to and utilization of youth friendly services is a challenge. In line with the HSTP, the ministry developed and disseminated the second National Adolescent and Youth health strategy (2016-2020) that commits to addressing Sexual reproductive health, Substance use, Communicable and non-communicable diseases, Nutrition, and injuries. In order to use an up-to-date data for monitoring progress, for the implementation of the strategy, a baseline statistics was also developed by using available secondary data including the 2016 DHS.
Adolescents and youth health service coverage and service Coverage:
Currently 44.7 of all health facilities provide youth friendly services and only 11% have at least one staff who received training on adolescent health services in the last two years. The region with the most facilities with trained staff are Tigray (20 percent), Amhara (17 percent) and SNNPR (16 percent). Gambela region had no facilities with staff trained in adolescent and youth health services and no facilities where the guidelines were available. Health centers were the type of facility which was most likely to have trained staff or available guidelines.More than 90% of married males from the rural areas reported that no health extension worker visited them for family planning consultation. Females, particularly those from the rural area, were least served
Mortality analysis
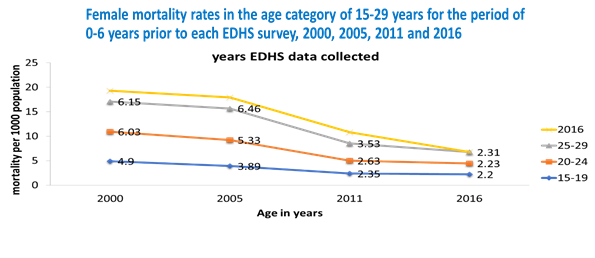
The overall mortality rate of any cause among Ethiopian adolescents and youth 10-29 years has Shown significant decline in the last decade. Specifically, female mortality rate (15-19 years) has dropped by more than half from about 4.89 in 2000 to 2.2 deaths per 1,000 Populations in 2016. The risk of mortality in females is known to increase as they enter the reproductive age because of pregnancy-related health problems. On the other hand, mortality of male adolescents and youth disproportionally increased to their female counterparts, due to exposure to road accidents and interpersonal violence. According to WHO 2015 report, estimated top five causes of death for boys aged 10-19 years in Ethiopia are lower respiratory infections, meningitis, diarrheal diseases, HIV/AIDS and road injuries. Among girls aged 10-14 years, lower respiratory infections, diarrheal diseases, HIV/AIDS, congenital anomalies, and road injuries are the main causes of death. Diarrheal diseases, maternal conditions, LRTIs, HIV/AIDS and epilepsy are causes of death among adolescent girls.
Morbidity
Sexual reproductive health, HIV and STIs
Evidences showed that the major sexual and reproductive health problems among adolescents and youth in Ethiopia are risky sexual practices, child marriage, early childbearing, unintended pregnancy, unsafe abortion and its complications and STIs including HIV. Data from the EDHS 2016 revealed that the median age at first marriage is 17.1 years among women and 23.7 years among men. According to EDHS reports, females were more likely to have sexual experience compared to males, which is probably due to earlier age of marriage among females. The median age at first sex was lowest among rural females (18 years), compared to 21 years among the other categories of adolescents and youth. While roughly 1 in 7 males (13-15 percent) had sex before the age of 18, 27 % of urban females and 52 % of rural females experienced first sex before the age of 18, which is likely due to earlier marriage among females Multiple sexual partners is also common among males than females. Nearly two-thirds (63 %) of urban males reported having had two or more lifetime partners compared to 44 % of rural males. ( AYH strategy: baseline statistic report)
HIV/AIDS and STIs among adolescents and youth
According to the EDHS 2016 report, the comprehensive knowledge of HIV among adolescents and youth, especially among rural females is very low. Only 16 % of rural females had comprehensive HIV knowledge, compared to 38 % of rural males, 39 % of urban females and 48 % of urban males. By contrast, large proportions of adolescents and youth knew where to get voluntary counseling and testing (VCT) for HIV. Over 90 % of urban youth knew where to get VCT, while 82 % of rural males and 69 % of rural females knew where to get the test. Urban females were the most likely to have undergone VCT (65 %), followed by urban males (59 %). In the same report, 5.4% of sexually active urban females and 3.2% of sexually active rural women had had a sexually transmitted infection (STI) in the last year.
Teenage pregnancy and child marriage
Many teenage pregnancies in Ethiopia occur within marriage. Although the legal age of marriage in Ethiopia is 18 years, 14.1% of girls are married by age 15, and 40.3% by age 18. Nationally, 13% of women age 15-19 have already given birth, and 2% are pregnant with their first child. Teenage childbearing is more common in rural than in urban areas (15 vs 5%), and also vary region to region; in Afar (23%) and Somali (19%) and; lowest in Addis Ababa (3%). Child marriage and teenage pregnancy has strong effects on the possibilities of girls to escape poverty.
Adolescent nutrition
Adolescence nutrition is an important public health problem among adolescents particularly to girls as they are often vulnerable to malnutrition because they are growing faster than at any time. It is also a time of menustration and important micronutrients like iron is highly needed for their growth. Chronic malnutrition and iron deficiency anemia are the most common forms of malnutrition among Ethiopian adolescent girls. 36% of non-pregnant adolescent girls aged 15-19 years are chronically malnourished (BMI <18.5) and the prevalence of anemia in the same group is 13%. At the same time, 2.2% of the girls and 0.3% of the boys in this age group are overweight. According to the national AYH baseline statistic report, nearly one quarter (23 %) of females aged 15 to 19 are considered underweight; 31 % of girls aged 15 to 19 in rural areas are underweight. In comparison, 17 % of urban females 15 to 29 are underweight. The urban population has moderate rates of obesity. 1 in 7 urban women (14 %) are considered overweight.
Substance use and mental health
The most common addictive substances used by adolescents and youth in Ethiopia are cigarettes, alcohol, and khat. According to EDHS 2016 report, 36.8 % of adolescent girls and 43.3 % of adolescent boys aged 15-19 years consumed alcohol six times or more for the last month. The national prevalence of Khat consumption among adolescents and youth is 51%; higher among males (56.5%) than females (36.6%). In Ethiopia, mental illness is the leading non-communicable disorder in terms of burden. At a prevalence of 12-25% childhood, mental illnesses make the highest burden of mental illnesses in the health sector.
Strategies and Guideline
- ADOLESCENT AND YOUTH HEALTH STANDARDS, IMPLEMENTATION GUIDELINE AND MINIMUM SERVICE DELIVERY PACKAGE
- NATIONAL GUIDE FOR STRUCTURED ON-THE-JOB TRAINING (SOJT) FOR REPRODUCTIVE HEALTH (RH)
- Minimum Service Package and Standards For Adolescents and Youth Health At Workplace in Ethiopia
- NATIONAL ADOLESCENTS AND YOUTH HEALTH STRATEGY(2021-2025)
- National Reproductive Health Commodity Security Strategy 2022- 2026
Program areas
- Advocacy and awareness creation program: National adolescents and youth health forum
- Youth responsive facilities through implementation of youth friendly health service packages
- Empowering younger adolescents through life skill education
- Access to quality health services
- Meaningful youth engagement
- Multispectral coordination and collaboration
The Family Health program core functions include:
- Develop and coordinate the implementation of policies and programs that promote the health of the family through efficient integrated health services in Ethiopia.
- Effective coordination with regional health bureaus, partners and other stakeholders to proactively contribute to overall family health in Ethiopia

Activities
- Scale up Family planning service uptake
- Integrated Catchment based Mentorship to selected health posts
- Postpartum Family Planning coverage
- Long Active Reversible Contraceptive coverage
- Advocacy and Health Care financing
- Family planning commodity security and supply chain management
- Awareness raising forums on Family Planning and SRH services
Guidelines and Standards
- FAMILY PLANNING SERVICE INTEGRATION NATIONAL IMPLEMENTATION GUIDELINE
- FP 2030 ETHIOPIA GOVERNMENT COMMITMENT
- National Family Planning Communication Guideline
Best practices and documentation
Media – News &Events
Upcoming events
Gallery of Activities
Press Release